Health Equity
Health Equity is when everyone has a fair and just opportunity to get their highest level of health.
BUHP’s purpose is: “We serve a diverse population at any stage of life, concerned for the health and wellbeing of their families, loves ones and themselves. We create the best experience ever through care and coverage. Rooted in the communities we serve; we make health care easier so life can be better.”
BUHP is committed to advancing quality and Health Equity for all.
- We seek to serve as a partner with community organizations and providers.
- We facilitate community integration and coordination.
- We are leaders in understanding and addressing issues of Health Equity.
Member Data
Banner University Health Plans (BUHP) actively collects data to better understand how our members use healthcare.
Why we collect this information:
- B – UFC/ACC wants to make sure that all our members get the best care possible.
- We want to better understand our members and identify their health needs.
- The data we collect includes race and ethnicity (REaL) data as well as sexual orientation and gender identity (SOGI) data.
- We ask for this information so that we can review the services that all members receive to make sure that everyone gets the highest quality of care.
- The data will be used to:
- Identify shortfalls in service for anyone.
- Identify gaps in our network.
- Identify training needs for our staff and network.
- Identify the need for new services.
- Identify the need for new providers.
- The data will NOT be used to:
- Authorize services.
- Deny services.
Language Needs
Banner University Health Plans focuses on methods and processes that helps members navigate the health care system, which can be increasingly difficult for members with Limited English Proficiency.
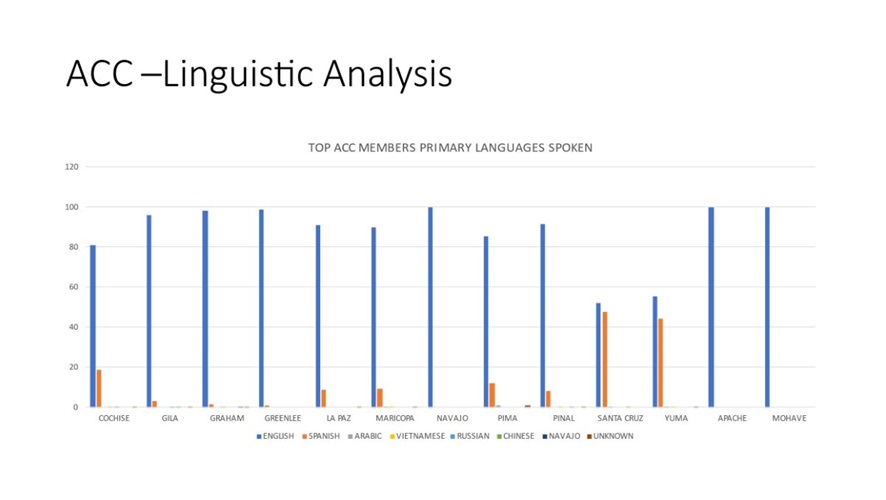
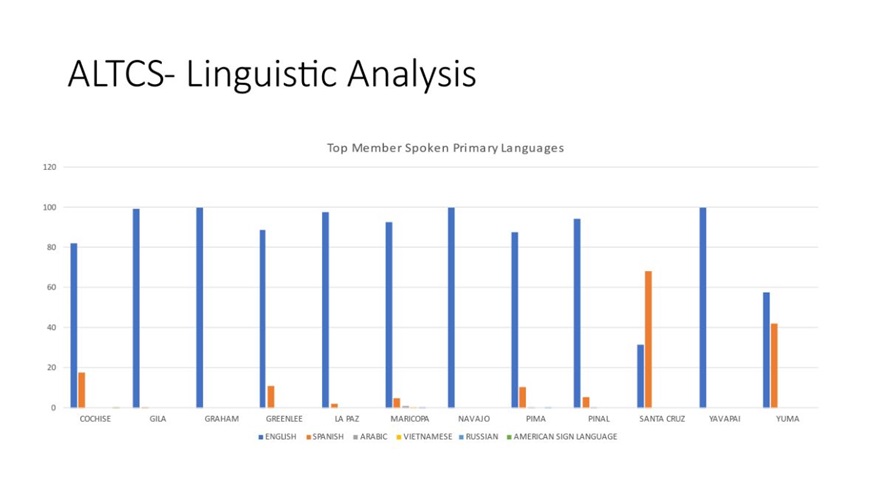
Serving Members by Speaking Their Language
Our health plan members speak lots of different languages. As of March 2024, 78% of members speak English. The following non-English languages are common and preferred among our members: Spanish, Navajo, Chinese, Vietnamese, Arabic, Filipino, Korean, French, German, Russian, Farsi, Assyrian, Serbo-Croatian, and Thai.
BUHP provides interpretation and translation services for members. If you need the following services, please contact our Customer Care Center at (800) 582-8686, TTY 711.
- Interpretation: SPOKEN word from one language to another.
- Translation: WRITTEN word from one language to another.
- Written materials in alternative formats.
Per the AHCCCS Contractor Operations Manual, Chapter 400, Policy 405:
- Individuals who do not speak English as their primary language and who have a limited ability to read, write, speak, or understand English may have limited English proficiency (LEP) and be eligible to receive language assistance for a particular type of service, benefit, or encountered as specified in 42 CFR 457.1207, 42 CFR 438.10.
- Individuals should have access to oral interpretation, translation, sign language, disability-related services, and provide auxiliary aids and alternative formats upon request, and at no cost.
- Translation and interpretation services need to be accurate, timely, and protect the privacy and independence of the individual with LEP. Translation and interpretation services shall be provided by a qualified interpreter/translator.
- Individuals are permitted to use an adult accompanying the individual with LEP for translation and/or interpretation 1) in an emergency when there is no qualified interpreter immediately available or 2) when the individual with LEP requests the accompanying adult to interpret or facilitate the communication, the accompanying adult agrees to provide the communication assistance, and reliance on the accompanying adult is reasonable under the circumstances. Individuals are not permitted to rely on a minor child for translation and/or interpretation except in an emergency when there is no qualified interpreter immediately available.
- All written materials for individuals shall be translated into Spanish regardless of whether materials are vital.
Health Disparities
Banner University Health Plans believes that understanding and addressing difference in health status, access and quality of care in communities we serve is critical to our mission of improving health outcomes for everyone.
Banner University Health plans has recently formalized two committee to help advance health equity, eliminate health disparities, and achieve the highest level of health for all people.
- Health Equity Committee
- Enrollee Advisory Committee
In addition, Banner University Health Plans has three additional structured forums that support health equity initiatives:
- Cultural Competency Committee
- Community Reinvestment Workgroup
- Neighborhood Advisory Councils
All four work collaboratively to advance health equity. Banner Health Plan has included each of their charters below and identify sponsor, membership, purpose, objectives, deliverable and cadence of meetings.
Health Equity Committee
A vital component of the Health Equity Plan, overseen by Banner University Health Plan’s Health Equity Committee is the use of multiple qualitative and quantitative data sources to identify disparities in healthcare. Identifying and monitoring such disparities with data sources can lead to the development of programs better aligned to meet the needs and preferences of diverse members. The Health Equity Committee is building out its strategies, monitoring the success and continue socializing the health equity initiatives with its providers, vendors, community-based organizations, and other stakeholders in the community.
Enrollee Advisory Committee
The Banner Medicare Advantage Dual Enrollee Advisory Committee (EAC) includes a reasonable representative sample of the plan’s membership, the communities, and the geographic service areas. The EAC will solicit input on, among other topics, ways to improve access to covered services, coordination of services, and health equity for Dual members, families and community stakeholders served by the Banner Medicare Advantage Dual Plan.
The EAC activities include, but not limited to, the following objectives:
- Receive and act on direct feedback to inform plan decision and improve plan processes.
- Resolving emerging issues.
- Meet the needs and preferences of members.
- Identify and address health equity barriers for underserviced member populations.
- Improve access to covered services and coordination of services.
- Addressing service and network challenges.
Cultural Competency Committee
The Cultural Competency Committee ensures health care services are delivered in a culturally competent manner. This includes member education, evaluating the cultural diversity of our members to assess needs and priorities, process improvement, and tracking of cultural competency training for providers, outsourced vendors, and health plan staff.
Duties of the Cultural Competency Program Committee include:
- Review regulatory reports or assignments (deliverables) with imminent due dates.
- Develop Cultural Competency training according to regulatory requirements.
- Assign subcommittees and/or workgroups for identified implementations, information research, process updates, etc.
- Tracking & Trending of any identifies Cultural Competency issues and document resolutions.
Community Reinvestment Workgroup
This workgroup carries out the following activities:
- Identify gaps in services to determine priorities for Community Reinvestment proposals.
- Develop and implement a process for the allocation of Community Reinvestment funds.
- Review and approve/reject community requests for funding and sponsorships.
- Review quarterly reports from Community Reinvestment awardees.
- Provide technical assistance to providers and community partners as it relates to the Community Reinvestment Program and application process.
Neighborhood Advisory Councils
Banner University Health Plans has developed the Healthy Community Dashboard to work with the Neighborhood Advisory Councils to achieve the following objectives:
- Identify the health conditions which are most prevalent in their community.
- Identify health inequities for these health conditions.
- Develop, implement and support interventions to address the health conditions and health inequities.
Health Related Social Needs
Health-Related Social Needs (HRSN) versus Social Determinants of Health (SDOH). SDOH are broader social conditions, HRSN are more immediate individual or family needs impacted by those conditions.
The term "Health-Related Social Needs" is sometimes used interchangeably with the Social Determinants of Health (SDOH), but an important distinction can be made. HRSN refers to the social and economic needs that individuals experience that affect their ability to maintain their health and well-being. They include things such as housing instability, housing quality, food insecurity, employment, personal safety, lack of transportation and affordable utilities, and more. SDOH, on the other hand, refers to the conditions in which people are born, grow, work, live, and age that are shaped by the distribution of money, power and resources and impacted by factors such as institutional bias, discrimination, racism, and more. In a way, disparities in HRSN can be understood as a result of the Social Determinants of Health. Addressing the conditions in which people live and their underlying factors is often out of scope for primary care practices. However, clinics can take steps to address the resulting health-related social needs through understanding which ones their unique patients face, referring them to local community services, partnering with community-based organizations, or coming up with other creative interventions.
Banner University Health Plan’s Health Equity Committee is collaborating closely with key Banner Health delivery stakeholders and other community-based partners to help drive utilization of Z codes for Banner University Health Plan members. Banner University Health Plan will look at different interventions such as increasing provider awareness, establishing performance and value-based agreements and educating coding professional. Z code categories Z55-Z65 are specifically used to document HRSN data (e.g., issues related to education, literacy, employment, housing, etc.) so the information can be used to can enhance quality improvement, track factors that influence health, and offer insight into existing health inequities.
ICD-10 z Codes for Health-Related Social Needs/SDOH
Education and Resources
Cultural Humility. EthnoMed
https://ethnomed.org/Aging Resources. American Public Health Association
https://apha.org/Topics-and-Issues/AgingDisability Resources. Centers for Disease Control and Prevention
https://www.cdc.gov/ncbddd/humandevelopment/health-equity.html
African American Resources. Centers for Disease Control and Prevention
https://www.cdc.gov/ncbddd/humandevelopment/health-equity.html
American Indian Resources. Northern Arizona University, Center for American Indian Resilience
https://in.nau.edu/cair/ai-health-equity-and-disparities/
Latino Resources. American Medical Association
https://www.ama-assn.org/delivering-care/population-care/hispaniclatinx-health-equity-educational-resources
LGBTQIA+ Resources. Center of Excellence, LGBTQ+ Behavioral Health Equity
https://lgbtqequity.org/resources/
Guiding Documents
CMS Health Equity Fact Sheet
https://www.cms.gov/files/document/health-equity-fact-sheet.pdf
NCQA Resources
https://www.ncqa.org/health-equity/
AHCCCS Health Equity Committee
Formally established in July 2020, the Health Equity Committee is tasked with understanding health disparities and developing strategies to ensure health equity for all AHCCCS members. The committee is responsible for overseeing and managing health equity considerations as they relate to policy, data, health plan oversight and emerging health care innovation strategies for over 2 million Arizonans. This committee is responsible for identifying health disparities among AHCCCS-eligible individuals and members by using AHCCCS utilization and quality improvement data to advance policy and/or contracting strategies to improve the health equity of AHCCCS’ populations and programs. This committee will communicate existing health equity strategies currently being implemented by the agency, identify needed improvements to existing strategies (if appropriate), develop and/or evaluate key metrics, and articulate future interventions aimed at eliminating health disparities. Committee Goals:
- Understand health disparities among AHCCCS members.
- Effectuate policy changes and support the implementation of strategies for positive improvement where known disparities exist, creating opportunities for the more equitable provision of services and supports.
- Raise the visibility of AHCCCS’ commitment to health equity and the strategies in place to ensure the equitable provision of services and supports.
- Improve health outcomes for AHCCCS members.
- Identify challenges and barriers that AHCCCS members have in accessing covered services